Diagnosis
This type of injury is one that is often under diagnosed, a mistake that can have detrimental implications to healing and recovery times (11). Functional testing will show obvious impairments, such as inability to perform a squat or single-legged hop, however this is characteristic of all ankle sprains (8). It is therefore imperative that after taking a thorough history and observing clinical signs that may be associated with the patient’s symptoms, a select few special tests be performed during the physical examination to support the hypothesised diagnosis of syndesmotic injury and rule out other differential diagnoses of lateral or medial ligament damage. Fundamental diagnostic imaging must also be utilised in order to determine if the extent of damage reached the bone.
Special Tests- These include tibial external rotation with ankle dorsiflexion, syndesmotic compression with maximum dorsiflexion and the Hopkins (Squeeze) test, (with external rotation test being the most reliable and the squeeze test being the least (11). These special tests are indicative of syndesmotic injury as they produce a clear positive result, while other ankle sprains are negative (9).
Special Tests- These include tibial external rotation with ankle dorsiflexion, syndesmotic compression with maximum dorsiflexion and the Hopkins (Squeeze) test, (with external rotation test being the most reliable and the squeeze test being the least (11). These special tests are indicative of syndesmotic injury as they produce a clear positive result, while other ankle sprains are negative (9).

1) Tibial External Rotation with Dorsiflexion-
Positive test if symptomatic pain is reproduced in the area of the syndesmosis- directly over the AITFL, PITFL or interosseus membrane (8).
Figure 3: External rotation test. For noting, additional ankle dorsiflexion will increase the patient's symptoms further. Taken from http://www.youtube.com/watch?v=9vWobLuXoQM. Click the link to watch a demonstration.
Positive test if symptomatic pain is reproduced in the area of the syndesmosis- directly over the AITFL, PITFL or interosseus membrane (8).
Figure 3: External rotation test. For noting, additional ankle dorsiflexion will increase the patient's symptoms further. Taken from http://www.youtube.com/watch?v=9vWobLuXoQM. Click the link to watch a demonstration.

2) Dorsiflexion-Compression Test-
In standing, the patient assumes a lunge position and moves into dorsiflexion. The movement is repeated with the therapist applying compression to the two malleoli. The test is positive for syndesmotic injury if this application of compression force decreases the pain experienced, or increases the ROM available.
Figure 4: Application of compression during dorsiflexion. Taken from http://www.youtube.com/watch?v=BmapwCfFRvU. Click the link to watch a demonstration.
In standing, the patient assumes a lunge position and moves into dorsiflexion. The movement is repeated with the therapist applying compression to the two malleoli. The test is positive for syndesmotic injury if this application of compression force decreases the pain experienced, or increases the ROM available.
Figure 4: Application of compression during dorsiflexion. Taken from http://www.youtube.com/watch?v=BmapwCfFRvU. Click the link to watch a demonstration.

3) Squeeze Test-
Positive test if compression of the tibia and fibula produces pain distally at the syndesmosis (8).
Figure 5: Application of the squeeze test. Taken from http://www.youtube.com/watch?v=uU5lNsA6_HA&feature=related. Click the link to watch a demonstration.
Positive test if compression of the tibia and fibula produces pain distally at the syndesmosis (8).
Figure 5: Application of the squeeze test. Taken from http://www.youtube.com/watch?v=uU5lNsA6_HA&feature=related. Click the link to watch a demonstration.

Severity of the injury can range from mild sprains (slight ligamentous tearing), moderate (mortise loosens) and severe (complete tearing of the ligaments and separation of the fibula and tibia in what’s known as diastasis). As shown in Figure 6, the distance from the distal tip of the fibula to the proximal point of tenderness can be measured as a prediction of the severity of the injury (8). To determine the extent of the damage, imaging is accepted normal practice and an essential component to the diagnostic process (15).
Figure 6: Measuring the length of tenderness
to predict severity of injury (8).
Figure 6: Measuring the length of tenderness
to predict severity of injury (8).
Radiography-
Syndesmosis injuries are defined by;
· More than five millimetres of widening of either the:
- anterior tibial tubercle-fibular space (Mortise view- see Figure 7).
- posterior tibial tubercle space or medial ankle joint space (AP view).
· or asymmetry of the tibiotalar crescents (Lateral view) (17).
Syndesmosis injuries are defined by;
· More than five millimetres of widening of either the:
- anterior tibial tubercle-fibular space (Mortise view- see Figure 7).
- posterior tibial tubercle space or medial ankle joint space (AP view).
· or asymmetry of the tibiotalar crescents (Lateral view) (17).

Figure 7: The arrows indicate the widening of the tibiofibular space that has occurred as a result of syndesmosis injury. On a normal, uninjured ankle, this space is less than 5mm (16).
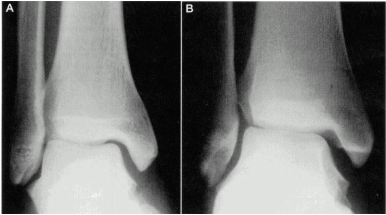
Stress views (x-rays taken during weight bearing) differentiate between stable ankle sprains and those involving diastasis (see Figures 8A and B) (15).
Figure 8: A=mortise view at rest, B=under stress. These are x-rays of the same ankle, illustrating the more apparent widening that occurs when a stress view is taken (15).
Figure 8: A=mortise view at rest, B=under stress. These are x-rays of the same ankle, illustrating the more apparent widening that occurs when a stress view is taken (15).
As previously mentioned, the likelihood of an associated fibula fracture or bony avulsion of the tibia is quite high with this type of injury (see Figures 9A and B for examples), and thus x-rays play an important role in determining treatment and management protocols for individual cases.

Figures 9A and B show examples of syndesmotic injury in conjunction to medial
malleolus and fibula fractures (11).
malleolus and fibula fractures (11).
MR Imaging- Typically used to grade ligamentous injuries, as it allows a more thorough assessment of the ligaments, but is also extremely effective for diagnosing avulsion injuries, as it will show fragments of bone adjacent to an irregular lateral or medial malleolus (3).
CT scan- Considered the most valuable technique to evaluate the syndesmosis congruency and fibula position (11). More sensitive than x-rays (which have been found to miss displacement of three millimetres half of the time) as they can detect syndesmosis widening of one millimetre (18).
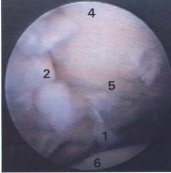
Arthroscopy- Usually the last option in patients contemplating surgery, see example image Figure 10.
Figure 10: Damaged posterior inferior tibiofibular (labelled 1) and interosseous (labelled 2) ligaments. A chondral fracture (labelled 5) has also been exposed at the posterolateral corner of the tibial plafond (19).